


Guidelines for the Treatment of Parkinson's Disease in China (Fourth Edition) (1)
2021-09-14
(Summary description)This study shows that there are no significant differences between bipolar type I and type II patients in many characteristics, such as family history of bipolar disorder, age of first depression and manic/hypomanic episodes, average manic/hypomanic episodes Duration, etc.; out of the 96 symptom items evaluated by the study, there was no significant difference in the proportion of 80 in the two groups.
(Summary description)This study shows that there are no significant differences between bipolar type I and type II patients in many characteristics, such as family history of bipolar disorder, age of first depression and manic/hypomanic episodes, average manic/hypomanic episodes Duration, etc.; out of the 96 symptom items evaluated by the study, there was no significant difference in the proportion of 80 in the two groups.
Yimaitong Guide Reading
This study shows that there are no significant differences between bipolar type I and type II patients in many characteristics, such as family history of bipolar disorder, age of first depression and manic/hypomanic episodes, average manic/hypomanic episodes Duration, etc.; out of the 96 symptom items evaluated by the study, there was no significant difference in the proportion of 80 in the two groups.
However, patients with bipolar type I have delusions (77.8% vs. 21.4%), hallucinations (55.6% vs. 14.6%), and certain psychotic manifestations (such as mysterious experiences) during manic/hypomanic episodes. , 61.1% vs. 24.3%) is significantly higher than the biphasic type II.
Whether hallucinations/delusions occur during mania/hypomanic episodes, this variable may be regarded as the simplest distinction point between biphasic type I and type II; this is also consistent with the historical concept that biphasic type I was once called "Manic-depressive psychosis." However, the severity, frequency, and duration of psychotic symptoms should also be considered.
The diagnostic criteria for bipolar disorder of DSM-5 and ICD-11 have certain limitations, which have caused troubles in clinical practice, such as the distinction between manic episodes and hypomanic episodes.
Take DSM-5 as an example: Diagnostic criteria A, except for the different duration requirements, other expressions are almost identical; Diagnostic criteria B, the two are exactly the same in terms of 7 items and the number of items required for diagnosis. In other words, mania and hypomania lack a clear symptomatic distinction point. The two may be identified through four dimensions, namely, the duration of symptoms, the degree of functional impairment, whether there are psychotic symptoms, and whether hospitalization is required.
ICD-11 distinguishes mania from hypomania in the same dimensions as DSM-5. For example, the duration of a manic episode is longer than that of hypomania, there are psychotic symptoms, etc.; the symptoms of bipolar II patients should not be severe enough to "cause significant damage" or require hospitalization. Even so, the actual clinical situation is often much more complicated, especially when it comes to retrospective diagnosis.
Research Introduction
AREDOC (Assessment, Revision and Evaluation of DSM and Other Operational Standards) working group is composed of well-known experts in the field of bipolar disorder worldwide. Among the 123 invited experts, 64 experts (from 14 countries) participated in the first phase of the working group’s study, which reviewed the limitations of DSM-5 and ICD diagnostic criteria for bipolar disorder, and proposed consensus improvements Suggest. The results of the first phase of the study were published in 2018 [1].
Based on the first phase of the study, the AREDOC working group carried out the second phase of the study [2], which discussed the following two topics based on patient-generated data: (1) Bipolar disorder as a whole (as opposed to unipolar depression) Define the standard; (2) How to better distinguish biphasic type I and type II. The second phase of the study was published online in Acta Psychiatr Scand. This article mainly introduces the findings on the second topic.
In short, the study included a total of 178 bipolar patients who could clearly recall their manic/hypomanic episodes, from Australia, Canada, the United States, Poland, and Singapore. The number of biphasic type I and type II was 74 and 104, respectively. People, with an average age of 43.1 years, 48.3% of men. These patients completed a structured questionnaire involving sociodemography, bipolar history and clinical features, family history, functional level and other information, and selected the symptoms that clearly existed at the time of their onset from 96 candidate symptoms. The first author of the study also recruited 33 patients with unilateral depression, and these patients also completed the same questionnaire with 96 symptom items.
Theoretically, if an item can describe the manic/hypomanic state well, then the item should have a high proportion in bipolar type I and type II patients, and a low proportion in depression patients. Is 0; if an item can distinguish mania from hypomanic episodes well, there should be a significant difference in the proportion of the item in bipolar type I and type II patients. The specific design of the study is detailed in the original text.
Research result
Of the 74 biphasic type I patients included in the study, 86.5% were classified as type I due to psychotic characteristics during manic/hypomanic episodes, 82.4% were classified as type I due to the need for hospitalization, and 73.0% It was included in this list because of severe symptoms. Seven (9.5%) patients with bipolar type I did not report any psychiatric experience, while among 104 patients with bipolar type II, 32 (30.8%) and 23 (22.1%) had delusions and hallucinations, respectively.
In terms of age, gender, marital status, years of education, and employment status, there were no significant differences between bipolar type I and type II patients, and between bipolar patients as a whole and depression patients.
Clinical features
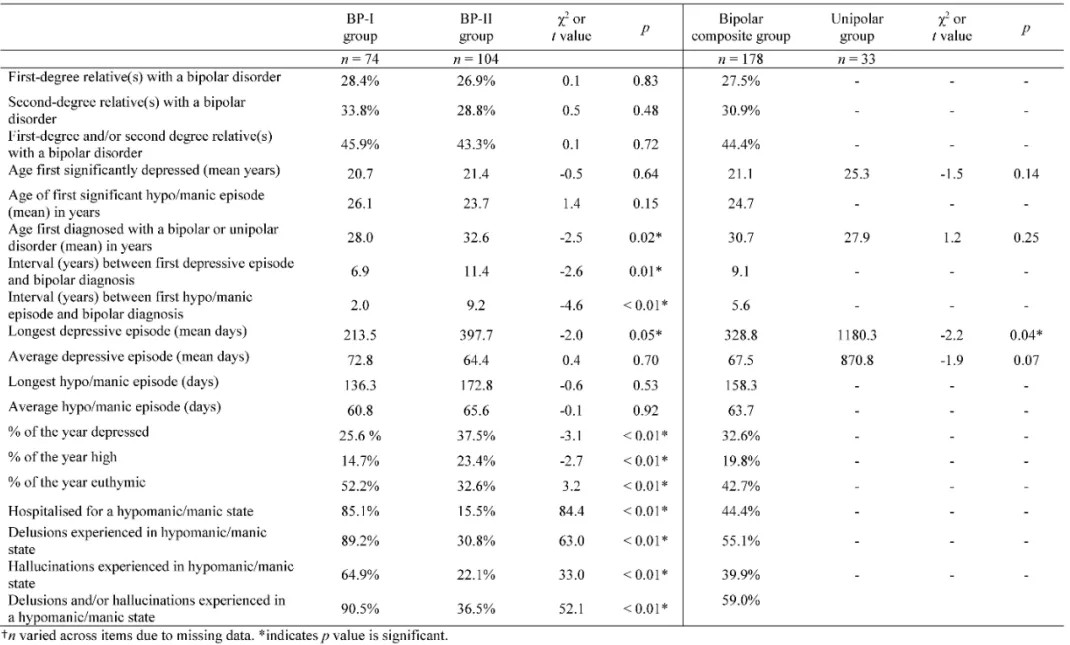
Family history of bipolar disorder, that is, the proportion of first-degree relatives, second-degree relatives, and first- and/or second-degree relatives suffering from bipolar disorder, there is no significant difference between bipolar type I and type II. The age of first depression and manic/hypomanic episode, the average length of depressive episode, the longest time of mania/hypomanic episode, and the average time of manic/hypomanic episode were also not significantly different between the two groups.
Table 1 Comparison of clinical characteristics of patients with biphasic type I, biphasic type II, and depression (Parker, G., et al. 2020)
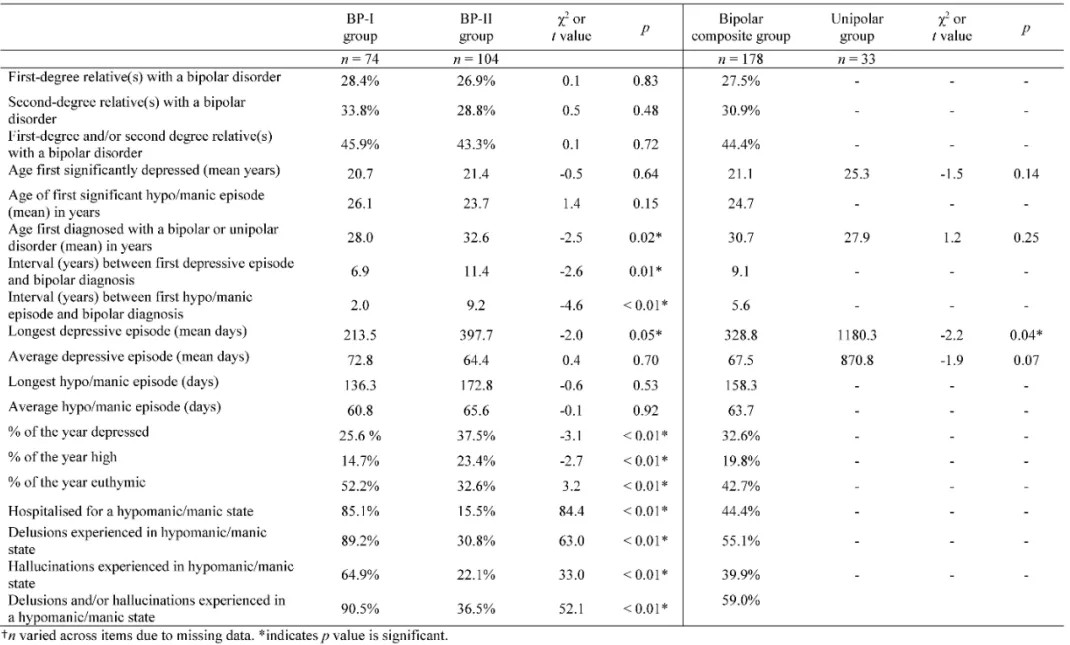
Patients with bipolar type I were significantly younger when they were first diagnosed with bipolar disorder (28.0 years vs. 32.6 years, p=0.02), and the time from first depressive episode to diagnosis was shorter (6.9 years vs. 11.4 years, p=0.01) ), the time from the first manic/hypomanic episode to diagnosis is shorter (2.0 years vs. 9.2 years, p<0.01).
The proportion of time that patients with bipolar type I are in a depressed state is significantly lower than that of bipolar type II (25.6% vs. 37.5%, p<0.01), and the proportion of time in a state of elevated mood is also significantly lower than that of bipolar type II (14.7% vs. . 23.4%, p<0.01), and the proportion of time with normal mood was significantly higher than that of biphasic type II (52.2% vs. 32.6%, p<0.01).
In addition, the proportion of patients with bipolar type I admitted to hospital for manic/hypomanic episodes was significantly higher than that of bipolar type II patients (85.1% vs. 15.5%, p<0.01), and delusions occurred during manic/hypomanic episodes (89.2 % vs. 30.8%, p<0.01), hallucinations (64.9% vs. 22.1%, p<0.01), delusions or hallucinations (90.5% vs. 36.5%, p<0.01) are also significantly higher than biphasic type II .
As a whole (bipolar type I + type II), the longest depressive duration of bipolar patients was significantly lower than that of unipolar depression (328.8 days vs. 1180.3 days, p=0.04).
functional level
Among patients with biphasic type I, 52.1% believe that mood disorders have caused significant functional damage to themselves, while medical treatment or hospitalization can help reduce adverse consequences; 46.6% believe that mood changes have brought about a certain degree of functional changes or work, interpersonal, and Bad consequences in social, but sometimes feel more productive or more creative. Among patients with biphasic type II, the above two proportions were 18.3% and 81.7%, respectively.
When directly asking patients "whether they feel that they have a higher level of function during mania or hypomania", the proportions of biphasic type I and type II patients who answered "yes" were high, and there was no significant difference between the two groups (75.7% vs. . 86.3%, p=0.11).
symptoms
Among the 96 symptoms involved in the study, almost all of the symptoms are present in bipolar patients in significantly higher proportions than in depression patients, and there is no significant difference in the proportion of most symptoms in bipolar I and II patients.
Table 2 16 symptoms with significant differences in the proportion of biphasic type I and type II patients (Parker, G., et al. 2020)
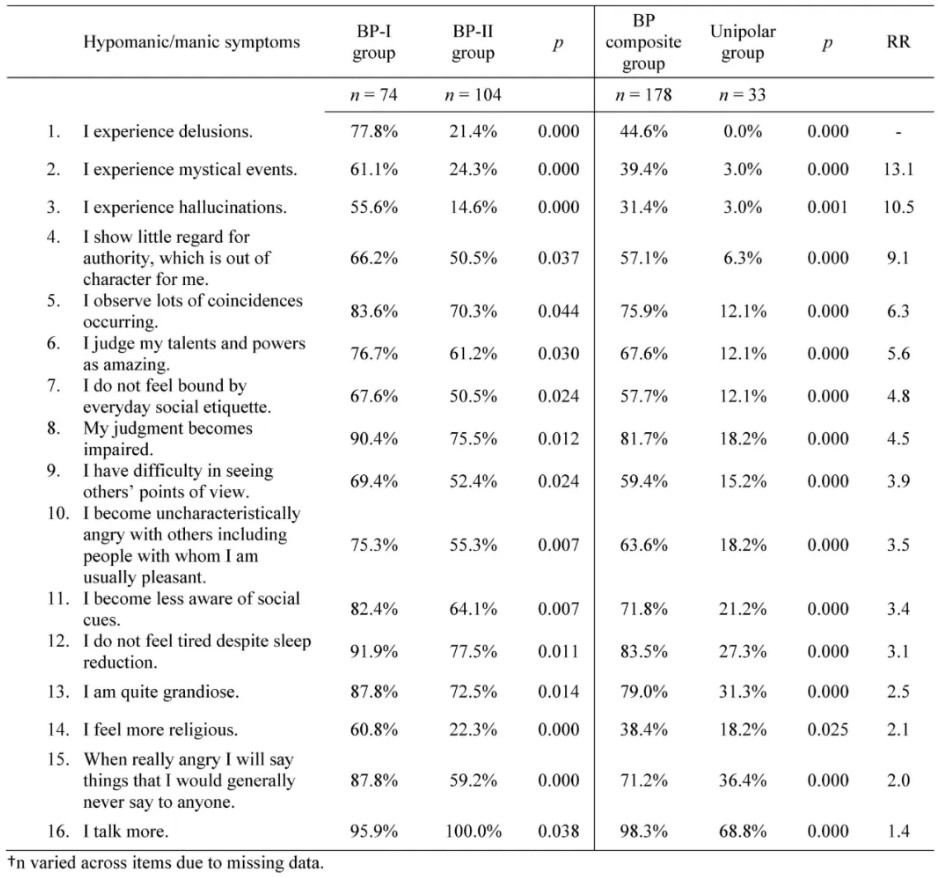
Specifically, there are 16 symptoms that differ between bipolar type I and type II, especially in patients with bipolar type I delusions (77.8% vs. 21.4%), hallucinations (55.6% vs. 14.6%), certain Some psychotic symptoms (such as mysterious experience, 61.1% vs. 24.3%) are significantly higher than biphasic type II.
in conclusion
There is no significant difference in many characteristics between the two-phase type I and type II. For example, the family history of bipolar disorder in the two groups was similar, and the age of onset of depression and manic/hypomanic episodes was similar. Although analysis shows that the proportion of time that patients with biphasic type I have a normal mood is significantly higher than that of biphasic type II, it is not clear whether this phenomenon is part of the natural course or the result of treatment. Among the 96 symptom items, most of them had no significant difference in the proportion of patients in the two groups.
The researcher pointed out that the simplest distinction between biphasic type I and type II may be a single variable, that is, "whether delusions and/or hallucinations have occurred"; this is also consistent with the historical concept—biphasic type I was once called "Manic-depressive psychosis." However, the actual clinical situation is often more complicated. For example, some patients have psychotic symptoms sometimes absent, and some patients have it at an early age and have not reappeared since then. The author recommends using the concept of dimensions to evaluate psychotic symptoms, including severity, frequency, and duration.
Literature Index:
1. Parker G, Tavella G, Macqueen G, et al. Revising Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, criteria for the bipolar disorders: Phase I of the AREDOC project. Aust N Z J Psychiatry. 2018;52(12):1173-1182. doi:10.1177/0004867418808382
2. Parker, G., Tavella, G., Ricciardi, T., Hadzi‐Pavlovic, D., Alda, M., Hajek, T., Dunner, D.L., O’Donovan, C., Rybakowski, J.K., Goldberg, J.F., Bayes, A., Sharma, V., Boyce, P. and Manicavasagar, V. (2020), Refined diagnostic criteria for the bipolar disorders: Phase Two of the AREDOC project. Acta Psychiatr Scand. Accepted Author Manuscript. doi:10.1111/acps.13218
Scan the QR code to read on your phone
Tel:025-86669187
e-mail:Office@Healsun.com
Address:Room 1616, Building F1, Intercity Space Station, No. 12 Jinlan Road, Jiangning District, Nanjing, China
Jiangsu Healsun Meical Co., Ltd. 苏ICP备19029369号-3

